
HEALTHCARE IT NEWS & BLOG
What 20 Years in Healthcare IT Taught Me About Client Trust
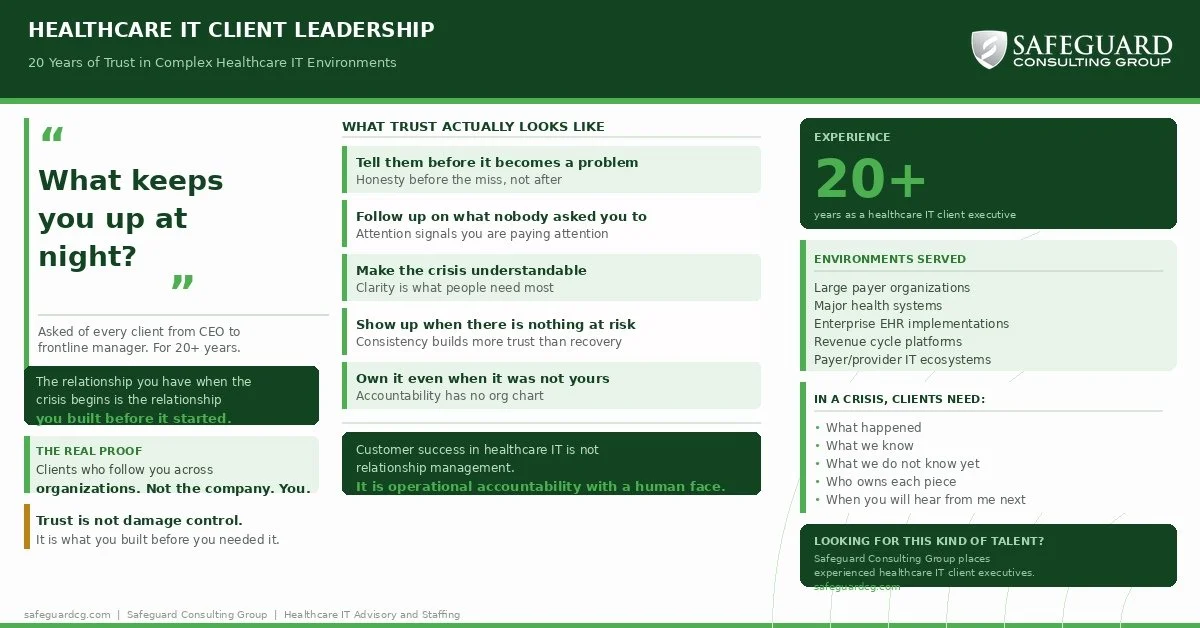
In healthcare IT, trust is not a soft skill. It is the operating currency when plans, systems, and timelines begin to fail. After 20 years as a client executive across payers and providers, here is what I have learned about what actually holds when everything else falls apart.
In healthcare IT, trust is not a soft skill. It is the operating currency when plans, systems, and timelines begin to fail.
For more than 20 years, I have worked with some of the most complex healthcare IT environments in the country: large payer organizations, major health systems, and enterprise implementations supporting thousands of users and critical operations.
I have been in the room when projects slipped, platforms failed to deliver, and executive leadership needed answers quickly. I have also been the person clients called when the situation escalated and they needed someone they trusted to take ownership.
The most important lesson I learned did not come from a customer success framework or a client management playbook.
The relationship you have when the crisis begins is the relationship you built before it started.
What a client executive actually does
The title can sound straightforward: one person the client goes to for everything.
In practice, the role is much more consequential.
A client executive owns the relationship, the outcome, and the trust the client places in the organization every day. That ownership extends beyond ticket queues, quarterly business reviews, renewal dates, and account plans.
When an implementation runs long, you explain what happened.
When a vendor or internal team drops the ball, you own the client experience even when the failure was not personally yours.
When senior leaders are asking why a platform is not delivering what was promised, you are the person sitting across the table from them.
You cannot delegate that moment. You cannot hide behind process, organizational boundaries, or someone else’s status report.
You are the face of the organization, and the only currency you have is the trust you earned before the meeting began.
The question that changes everything
Early in my career, I developed a habit that shaped nearly every client relationship that followed.
Whenever I began working with a new client, whether I was speaking with a CEO, an operational leader, or a frontline manager, I asked the same question:
“What keeps you up at night?”
Not: What are your project goals?
Not: What does success look like for this engagement?
Not: What are your key performance indicators?
Those questions have value, but they often produce answers that have already been filtered through contracts, project plans, and organizational language.
“What keeps you up at night?” gets to the real concern.
It reveals the issue the client is personally accountable for, the risk they believe others may be underestimating, or the operational problem that never made it into the statement of work.
It also sends an immediate signal: I am not here simply to execute a process. I am here to understand what genuinely matters to you.
I have asked that question of executives at large health systems, payer organizations, and enterprise technology companies. The answers are always different, but they consistently reveal where trust must be earned.
Trust is built before the crisis
Many customer success models treat trust as something to repair after a problem occurs.
Send the right email. Schedule the right call. Escalate appropriately. Provide an action plan. Close the loop.
Those steps matter, but they are not trust. They are service recovery.
Real trust is built during the quieter moments.
It is built when you tell a client something they do not want to hear before it becomes a larger problem.
It is built when you follow up on an issue nobody reminded you to track.
It is built when you acknowledge that a timeline is slipping instead of waiting until the slip becomes a missed commitment.
It is built when you show up consistently, not only when the account is at risk or the renewal is approaching.
Trust rarely comes from one dramatic act. It comes from hundreds of smaller interactions in which you demonstrated that you were paying attention, that you would be honest, and that the client’s outcome mattered to you.
When the crisis eventually comes—and in complex healthcare IT environments, it usually does—the client remembers those interactions.
They may not expect perfection. They do expect the truth, a clear plan, and confidence that someone is genuinely accountable.
Operational clarity is a trust signal
One of the most valuable things a client executive can do is make a complicated situation understandable.
Healthcare IT environments are genuinely complex. They may include multiple system integrations, payer configurations, clinical workflows, revenue-cycle dependencies, data exchanges, security requirements, and regulatory obligations.
When something breaks, the cause is rarely simple, and the resolution is rarely immediate.
Clients understand complexity. What they cannot tolerate is silence, vagueness, or the feeling that nobody is actually in charge.
In a difficult situation, a client executive should be able to say:
* Here is what happened.
* Here is what we know.
* Here is what we do not know yet.
* Here is who owns each workstream.
* Here is what happens next.
* Here is when you will hear from me again.
That is a trust signal.
Not because the issue has already been resolved, but because the situation has been made manageable.
Operational clarity under pressure is one of the most important capabilities a senior client executive brings to a relationship. It does not come from a script. It comes from experience, discipline, and the ability to remain accountable when the environment becomes uncertain.
Why healthcare makes this harder
Every industry depends on client relationships. Healthcare IT raises the stakes.
The systems being supported may affect patient care, clinical documentation, claims processing, revenue integrity, regulatory compliance, and a clinician’s ability to perform their job.
When those systems fail, the impact extends beyond a business inconvenience.
Healthcare leaders are also operating under extraordinary pressure. They are managing workforce shortages, margin compression, regulatory change, cybersecurity threats, technology complexity, and rising expectations from patients and employees.
When they place trust in a technology partner, they are not simply trusting that company with a contract. They are trusting it with outcomes for which they are personally accountable.
That changes how a client executive must show up.
The tolerance for ambiguity is lower. The need for a reliable, accountable point of contact is higher. Communication must be direct. Ownership must be visible. Commitments must be credible.
The relationship has to be grounded in something more durable than good service recovery.
It has to be grounded in trust.
The proof is in who follows you
After more than 20 years in healthcare IT, I have found that the clearest evidence of trust is not a renewal, a satisfaction score, or a successful quarterly review.
It is the client who follows you.
It is the executive who moves to another organization and calls you again.
It is the health system leader you worked with years earlier who reaches out because they are facing something difficult and want someone they trust in the room.
That does not happen because you managed an account efficiently.
It happens because you showed up honestly, consistently, and with genuine interest in what mattered most to them—not only when a contract was up for renewal, but every time you were in the room.
What this means for healthcare IT organizations
Healthcare IT organizations often measure renewals, satisfaction, expansion, retention, and referenceability.
Those are important outcomes, but they are outputs of trust. They are not the activities that create it.
Trust is built through:
* consistency before the account is at risk,
* honesty before a missed commitment becomes unavoidable,
* ownership when responsibilities cross organizational boundaries,
* and operational clarity when the situation is difficult.
The clients who remain, expand, and refer others do so because they believe the people serving them will tell the truth, take responsibility, and remain present when the work becomes hard.
That does not happen by accident.
It is a discipline.
And after more than two decades in healthcare IT, it is the one thing I have consistently seen hold when everything else begins to fall apart.
At Safeguard Consulting Group, we help healthcare organizations strengthen the client-facing teams responsible for these relationships. The best client executives do more than manage accounts. They create clarity, accountability, and trust when the stakes are highest.
Contact: info@safeguardcg.com
85% of Epic Clients Are Using Epic AI. The Gap Now Is Who's Actually Getting the Return.
85% of Epic clients are now using Epic AI tools. But adoption was never the hard part. The health systems seeing real return built workflow and governance around these tools before they turned them on. Most didn't. Here's what that gap actually looks like.
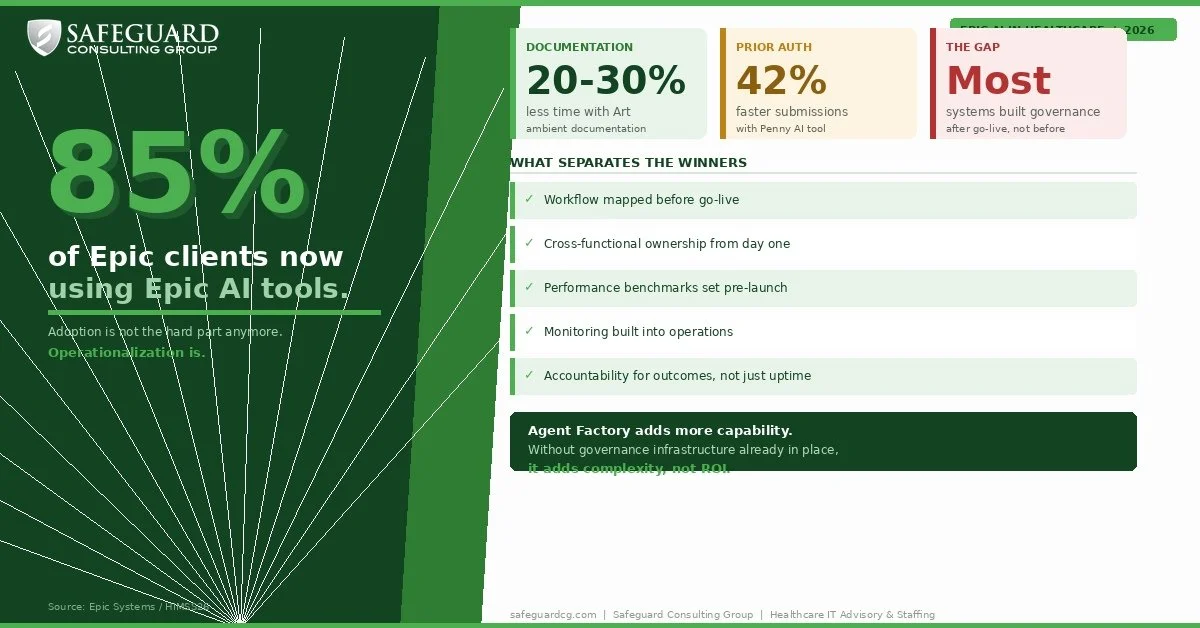
85% of Epic clients are now using Epic AI tools. That number gets repeated a lot right now. But it's the wrong headline.
Adoption stopped being the hard part a while ago. The tools work. Art is cutting clinical documentation time 20 to 30% at health systems that deployed it well. Penny is cutting prior authorization submission time by 42% at some organizations. Discharge summaries that used to take 15 minutes are getting done in under five. The capability is real and it is improving fast.
What's actually separating health systems right now is not whether they turned the tools on. It's what they built around them before they did.
Adoption is not the same as operationalization
Turning on an Epic AI tool is not an implementation. It's a starting point.
The health systems seeing real return on these tools did the work before go-live. They mapped how Art actually changes a physician's documentation workflow, not in theory, but in practice. They figured out who owns the tool's performance after launch. They set benchmarks so they'd know within 60 days whether it was performing or just running. They trained staff on the workflow change, not just the software feature.
The health systems struggling are the ones that turned tools on because the capability was there and the board was asking about AI. Six months later they have adoption metrics that look fine and ROI that's hard to find.
That gap is not a technology problem. It's a planning and governance problem.
Agent Factory makes this more urgent, not less
Epic announced Agent Factory at HIMSS26, giving health systems the ability to build and deploy their own AI agents across clinical and operational workflows. More capability, more flexibility, more control.
Also more complexity. More decisions about who owns what, who monitors what, and what happens when something drifts or goes wrong.
The organizations that are going to get the most out of Agent Factory are the ones that already have governance infrastructure in place from their existing AI deployments. The ones that don't are about to add a longer to-do list without the structure to manage it.
What good looks like right now
The health systems capturing real ROI from Epic AI share a few things in common. They treated AI deployment like an operational project, not an IT project. They kept experienced clinical and operational people in the loop on workflow design, not just the technical implementation team. They built monitoring into the process before go-live, not after. And they have someone accountable for outcomes, not just uptime.
That last point matters more than most organizations realize. A tool that runs is not the same as a tool that performs. In healthcare, the difference shows up in documentation quality, denial rates, staff adoption, and eventually in revenue.
The question worth asking right now
If your health system is live on Epic AI tools, the most useful question is not how many features are enabled. It's where you are actually seeing measurable return, and where the tool is still just a feature nobody fully operationalized.
If the answer to the second part of that question is uncomfortable, that's worth paying attention to before you add more capability on top of a foundation that hasn't been validated yet.
At Safeguard Consulting Group we work with health systems at both stages. Whether you need experienced resources to support an AI workflow deployment or help assessing whether what you've already built is performing the way it should, we are happy to have a direct conversation about what makes sense for your situation.
Reach out at info@safeguardcg.com.

Epic Now Controls 57% of US Hospital Beds. Here's What the 2026 EHR Scorecard Actually Tells Us.
The US EHR market is consolidating fast. Epic is winning. Oracle Health is losing ground. And health systems that have not made a decision yet are watching carefully while redirecting their capital somewhere else. Here is what the 2026 numbers actually say.
The US EHR market is consolidating. If you work in healthcare IT, the direction of travel is no longer a question.
Epic is winning. Oracle Health is losing ground fast. And health systems that have not made an EHR decision yet are watching carefully while quietly redirecting their capital somewhere else.
Here is what the numbers actually say.
Epic's Dominance
Epic now holds 43.7% of all US acute care hospitals and 56.9% of all hospital beds. In 2025 alone, the company added 77 hospitals and 18,679 beds. Since 2021, Epic has gained a net 568 hospitals.
Every large health system that made an EHR decision in 2025 chose Epic. Both enterprise purchases involving more than 10 hospitals went to Epic. No other vendor was chosen in a decision involving more than three multispecialty hospitals.
MyChart now has over 200 million activated patient accounts. Epic holds records for 325 million patients. The company is still private, still headquartered in Verona, Wisconsin, and still run by founder Judy Faulkner.
The growth is not accidental. Epic has built a platform that large health systems find difficult to leave and smaller systems are increasingly choosing to join through its Community Connect program. The network effect is real and it is compounding year over year.
The Oracle Health Decline
Oracle Health lost 56 hospitals and 14,676 beds in 2025. That is the third consecutive year of major net losses. Since 2021, Oracle has shed a net 173 hospitals.
The customer base has grown increasingly unstable. About 30% of sampled Oracle Health customers say the platform is not part of their long-term plans. Another 35% are considered at risk of leaving. That means roughly two thirds of the Oracle customer base is either actively planning to leave or watching closely for a reason to.
Customer satisfaction with the Millennium platform has continued to slide following repeated layoffs, restructuring, and strategic uncertainty since Oracle's acquisition of Cerner. In the 2026 Best in KLAS report, Millennium ranked as the lowest-scoring acute care EHR across large, midsize, and small organizations.
Major health systems including UAB Medicine, Indiana University Health, and MedStar Health have announced plans to move to Epic.
The one thing Oracle has working in its favor in 2026 is its new AI-enabled EHR platform. Whether it lands well with existing customers will go a long way toward determining whether the bleeding slows or accelerates.
The VA Situation
The Oracle Health story cannot be told without the VA.
The VA signed a $10 billion contract with Cerner in 2018 to modernize its EHR across 170 medical centers. Oracle acquired Cerner in 2022 and inherited the project. The contract has since been revised to over $16 billion, with some lifecycle cost estimates from lawmakers running as high as $37 billion.
As of now, 10 of the VA's 170 medical centers are live on the new system. The rollout was paused for nearly three years due to patient safety concerns, technical failures, and usability problems. VA restarted deployments in April 2026 with four simultaneous go-lives in Michigan, a new approach after previous single-site rollouts struggled badly.
The target is full deployment by 2031. The GAO has flagged 16 of 18 outstanding recommendations as not yet implemented. Employee groups at recently deployed sites report many of the same problems that caused the original pause.
It is the largest IT implementation in federal government history. The outcome still matters for Oracle Health's credibility in the broader market.
The Rest of the Market
MEDITECH holds 14.7% of acute care hospitals and is showing the strongest legacy customer retention in the market right now. 84% of their legacy customers are migrating to Expanse rather than leaving for a competitor. That is a quiet stability story that does not get enough attention.
The ambulatory market looks different. Epic leads with 19.5% share. eClinicalWorks follows at 11.9%. athenahealth holds 6.9%. The ambulatory space remains more fragmented, with vendors carving out specific niches in independent practice, specialty care, and outpatient settings where Epic's cost and complexity are harder to justify.
The Slowdown Nobody Is Talking About
EHR purchasing decisions dropped roughly 40% in 2025 compared to 2024 and nearly 50% compared to 2023.
That is not a vendor story. That is a market story. Health systems are not standing still. They are redirecting capital toward AI tools, operational efficiency platforms, and technologies with faster financial returns. The big EHR replacement cycle has slowed significantly, and organizations still weighing a move are largely waiting to see what Oracle's next chapter looks like before they act.
Why This Matters Beyond the Numbers
The EHR vendor controls the clinical workflow. It shapes what data you can access, what integrations are possible, and what your technology roadmap looks like for the next decade.
Organizations on stable platforms are building toward AI, workflow automation, and deeper interoperability. Organizations on uncertain platforms are managing vendor risk, watching peers leave, and trying to figure out the right moment to make a move.
That gap will widen over the next few years, not narrow.
How Safeguard Can Help
Whether your organization is navigating an EHR transition, supporting a go-live, or building the operational and IT infrastructure to get the most out of the platform you are already on, Safeguard Consulting Group can help.
We work with health systems across payer and provider environments to provide experienced consulting and staffing support at every stage of the technology lifecycle. EHR transitions are complex, long-cycle projects that require the right people at the right time. We help you find them and deploy them effectively.
If your organization is in the middle of an EHR decision or preparing for what comes next, we are happy to have a direct conversation about what support actually looks like.
Reach out at info@safeguardcg.com.
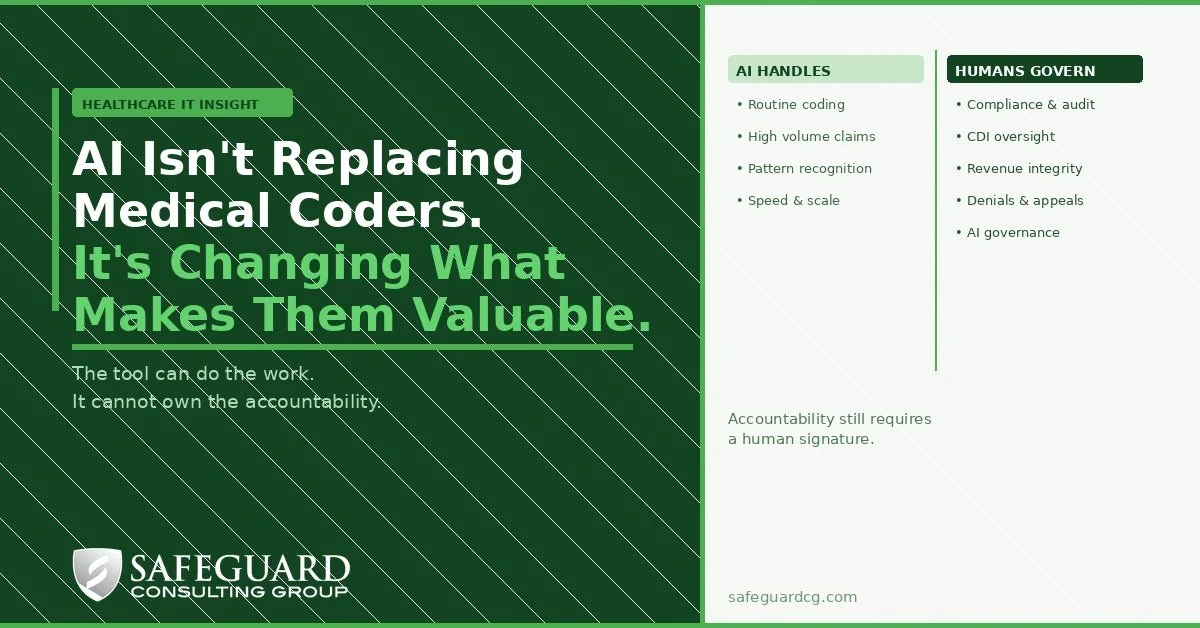
AI Isn't Replacing Medical Coders. It's Changing What Makes Them Valuable.
The healthcare industry keeps asking the wrong question. Instead of asking whether AI will replace medical coders, we should be asking who is responsible when the code is wrong. That question changes everything.
The healthcare industry keeps asking the wrong question.
Every few months another article drops about AI replacing medical coders. Productivity tools are getting smarter. Autonomous coding platforms are improving. The anxiety inside HIM departments and revenue cycle teams is real.
But the question nobody is asking loudly enough is this: who is responsible when the code is wrong?
That question changes everything.
What AI is actually doing to coding work
AI is genuinely capable of identifying diagnoses, procedures, and coding patterns at a speed and volume no human team can match. Routine coding work — high-volume, low-complexity claims — will increasingly be handled by automated tools. Productivity per coder will go up. Some production coding roles will shrink over time.
That part is true and worth saying plainly.
But automating the work is not the same as eliminating the judgment. In medical coding, the judgment is where the real liability lives.
A miscoded claim does not just result in a denial. It can trigger a payer audit, a compliance review, a fraud and abuse inquiry. It can affect quality scores, risk adjustment accuracy, and reimbursement at scale. When that happens, someone has to answer for it. An AI platform cannot sit in front of a payer or a regulator and defend a coding decision.
A human has to do that.
Where the value is actually shifting
The coders who will struggle are the ones whose entire value is production volume. Getting through as many charts as possible per day. AI will do that faster and cheaper.
The professionals who will thrive are the ones who can do what AI cannot: evaluate documentation quality, identify risk, defend decisions, govern the tools doing the work, and catch what the model missed or got wrong.
The highest value work in medical coding is moving toward:
Compliance and audit. Reviewing AI-generated coding decisions for accuracy, risk exposure, and regulatory alignment.
Clinical Documentation Improvement. Working with physicians upstream to ensure documentation actually supports the codes being assigned. AI cannot do that without experienced human judgment in the loop.
Revenue Integrity. Identifying patterns where coding decisions are affecting reimbursement in ways that may not be visible at the claim level.
Denials and Appeals. When a payer pushes back, you need someone who can build and defend the clinical and coding argument. That is not an AI job.
AI-Assisted Coding Governance. Someone has to own the rules the model is coding by, monitor its performance, catch drift, and escalate when something looks off. That role requires deep coding expertise combined with enough operational judgment to govern a system, not just use one.
This is the same governance problem showing up everywhere
If this sounds familiar, it should. It is the same pattern playing out across every AI deployment in healthcare right now.
Organizations that treat AI as a production replacement - buy the tool, turn it on, reduce headcount — are the ones that will face the audit, the denial spike, or the compliance gap they did not see coming.
Organizations that treat AI as a production accelerator — deploy it to handle volume, keep experienced humans governing the output, validating the logic, and owning the risk — are the ones building something durable.
Medical coding is not a special case. It is a clear example of a principle that applies across healthcare AI: the tool can do the work, but it cannot own the accountability.
Accountability still requires a human signature.
What this means for healthcare leaders
If you are a revenue cycle or HIM leader evaluating AI coding tools right now, the deployment question is only half the equation. The governance question is the other half.
Who is reviewing the model's output? What are your accuracy benchmarks and who owns them? How are you catching drift before it shows up in your denial rate or an external audit? What does your escalation path look like when the model gets it wrong?
If you do not have clear answers to those questions, you are not ready to reduce your experienced coding staff. You may be ready to redeploy them.
The coders who understand documentation, compliance, audit risk, and revenue integrity are not being replaced by AI. They are becoming the people responsible for making sure AI does not create a problem your organization has to explain to a payer or a regulator.
That is not a lesser role. In many organizations it is a more important one.
At Safeguard Consulting Group we work with healthcare organizations navigating exactly this kind of transition. Building the operational and governance infrastructure to deploy AI responsibly without creating risk in the process. If you are working through this, we are happy to have a direct conversation.
Reach out at info@safeguardcg.com.

What Healthcare IT Leaders Get Wrong When Deploying AI
Healthcare organizations are under real pressure to do something with AI. Boards are asking about it. Competitors are announcing it. Vendors are pitching it hard. Most of them are going to regret how they did it. The problem is almost never the tool — it's everything around it.
Healthcare organizations are under real pressure to do something with AI. Boards are asking about it. Competitors are announcing it. Vendors are pitching it hard. And so a lot of organizations are moving fast — buying tools, launching pilots, announcing initiatives.
Most of them are going to regret how they did it.
That's not a knock on AI. The technology works. The problem is almost never the tool. It's everything around the tool — how it gets bought, who owns it, how it gets monitored, and what happens when something goes wrong.
After two decades working inside healthcare IT across payers and providers, one thing stands out about AI deployments right now — the failures are rarely about the technology. Here's what's actually happening.
Buying the demo instead of validating the reality
Every AI vendor has a great demo. Clean data, favorable use case, reference site that looks nothing like your environment.
Then you sign the contract, and the tool hits your actual EHR configuration, your actual patient population, and your actual workflows. The gap between what was promised and what's performing starts to show.
This is not a technology problem. It's a validation problem. Before you commit to anything, test the tool against your data, in your environment, against the specific use case you're actually trying to solve. Not the vendor's preferred scenario. Yours.
If a vendor won't support that kind of validation before you sign, that tells you something.
Handing it to IT and calling it done
AI gets routed to IT because it's a technology purchase. That's the wrong frame.
AI in healthcare is a clinical and operational project that happens to run on technology. When IT owns it in isolation, you end up with a tool that runs but doesn't perform. Physicians don't trust outputs they weren't involved in validating. Compliance discovers audit exposure after the fact. Revenue cycle finds out about billing workflow impacts when claims start denying.
The organizations getting this right build cross-functional ownership from day one. IT manages the infrastructure. Clinical leads validate the logic. Compliance sits at the table. Operations owns the workflow integration. Someone at the leadership level is accountable for outcomes — not just uptime.
Without that structure, you have a running tool and a performance problem nobody owns.
Treating go-live like the finish line
Deployment is not the end of the project. It's where the real work starts.
AI models drift. Patient populations shift. Regulatory updates change what the model is optimizing for. A tool that performed well at launch can quietly degrade for months, and in healthcare you usually find out the hard way — a denied claim, a clinical decision that doesn't hold up, a compliance gap that surfaces during a review.
You need defined performance benchmarks before you go live. You need a monitoring process built into operations. And you need a clear escalation path for when something looks off. If your vendor doesn't have a structured answer for how post-deployment performance gets tracked, that's worth surfacing before you sign anything.
Skipping governance because you're moving fast
The pressure to show AI progress is real. I'm not dismissing it. But speed without governance is how you build liability you didn't anticipate.
Governance doesn't have to be slow. A functional starting point is straightforward: know what's running, who owns each tool, how decisions are being made, and how you'd explain it in an audit. That's not a six-month framework project. It can be stood up quickly if you're intentional about it.
The organizations that skipped governance are now quietly rolling back tools they spent months deploying. Getting it right on the front end is significantly cheaper than unwinding it on the back end.
The data problem nobody wants to admit
Healthcare data is messy. That's not a criticism — it's the reality of an industry that has been layering systems on top of each other for thirty years.
AI runs on data quality. If your source data has gaps, inconsistencies, or reconciliation problems across platforms, the model amplifies those problems. It doesn't correct them.
Before you deploy any AI tool that touches clinical or financial workflows, you need an honest assessment of your data environment. What does the model actually need to function? Where does that data live? How clean is it? What happens when it's wrong?
Skipping this step doesn't save time. It moves the problem downstream where it costs more.
What this means practically
If you're early in AI deployment, the most valuable thing you can do right now is slow down long enough to validate before you scale. Test against your data. Build cross-functional ownership. Define what success looks like before you go live — not after.
If you're already deployed and some of this sounds familiar, an honest assessment of your current posture is worth doing now. Before a compliance review does it for you.
At Safeguard Consulting Group, we work with healthcare organizations at both stages. Whether you need experienced resources to support an AI initiative or help assessing what you've already built, we're happy to have a direct conversation about what makes sense for your situation.
Reach out at info@safeguardcg.com.

Why IT Augmentation Beats Full-Time Hiring in Healthcare Right Now
Healthcare IT leaders are being asked to do more with less. Budgets are under pressure. Workforces are stretched. And the list of priorities keeps growing: EHR optimization, AI implementation, cybersecurity hardening, regulatory compliance. Something has to give, and for a lot of organizations, the answer has been to hire full-time staff. That approach looks straightforward on paper. In practice, it creates more problems than it solves.
Healthcare IT leaders are being asked to do more with less. Budgets are under pressure. Workforces are stretched. And the list of priorities keeps growing: EHR optimization, AI implementation, cybersecurity hardening, and regulatory compliance. Something has to give, and for a lot of organizations, the answer has been to hire full-time staff. That approach looks straightforward on paper. In practice, it creates more problems than it solves.
The healthcare IT talent market is competitive and slow. A full-time hire takes months to source, interview, onboard, and get up to speed. By the time they're contributing at full capacity, the need may have already shifted. You've committed to salary, benefits, and overhead for a role that was built around a specific initiative, not a permanent function.
Augmentation is a different model entirely, and right now it's the smarter play for most healthcare organizations.
What Augmentation Actually Means
IT augmentation isn't a staffing agency sending you a warm body to fill a chair. Done right, it means bringing in experienced professionals who are ready to work from day one, scoped to the specific need, and accountable to your outcomes.
You're not managing a search process. You're not carrying long-term overhead. You're adding capacity exactly where you need it, for exactly as long as you need it.
That flexibility matters more in healthcare IT than almost any other sector. Projects don't always land on schedule. Regulatory timelines shift. A go-live that was six months out becomes three months out. Augmentation lets you respond to that without restructuring your team.
Where Full-Time Hiring Works Against You
The cost of a full-time healthcare IT hire goes well beyond salary. Benefits, payroll taxes, recruiting fees, onboarding time, and management overhead add up fast. For specialized roles like EHR analysts, integration engineers, or compliance specialists, you're often looking at total costs that run 30 to 40 percent above base compensation.
And if the project ends or the scope changes? You're either carrying headcount you no longer need or going through a difficult and expensive reduction process.
Augmentation removes that risk. You pay for the expertise you need, for the duration you need it, and when the engagement ends, you're not left managing a staffing overhang.
The Expertise Gap Is Real
One of the most overlooked benefits of augmentation is access to specialization that's hard to build and maintain in-house. Healthcare IT is not a monolithic skill set. EHR implementation, interoperability, revenue cycle optimization, cybersecurity, data governance, AI integration — these are distinct disciplines, and expecting one or two full-time hires to cover all of them is unrealistic.
Augmentation lets you bring in the right expertise for the right problem. An organization preparing for an Epic upgrade doesn't need a permanent Epic specialist on staff forever. They need one for the duration of that project, executing at a high level, and accountable to a clear scope.
That's exactly what Safeguard Consulting Group delivers. We place experienced healthcare IT professionals into organizations that need to move fast without the overhead of a full hiring cycle.
When to Make the Call
If any of these sound familiar, augmentation is worth a serious look:
You have a project with a defined timeline and no internal bandwidth to execute it.
You need a specialized skill set that doesn't justify a permanent hire.
You're facing a compliance deadline, and your current team is already at capacity.
You've been trying to fill a role for months, and the right candidate hasn't shown up.
You need flexibility to scale up or down based on how the year unfolds.
The organizations getting the most out of their IT investments right now are not necessarily the ones with the largest internal teams. They're the ones making smarter decisions about where to build permanently and where to bring in targeted expertise.
The Bottom Line
Healthcare IT is not getting simpler. The demands on your team are only going up. Building a permanent headcount strategy around a constantly shifting project landscape is expensive, slow, and inflexible.
Augmentation gives you speed, specialization, and cost control. For most healthcare organizations right now, that combination is hard to beat.
If you're evaluating your IT staffing strategy, we're happy to have a direct conversation about what makes sense for your situation.
Ready to talk through your IT staffing needs? Contact Safeguard Consulting Group at info@safeguardcg.com.

AI Governance in Healthcare: Why You Can't Afford to Skip It
AI is in your clinical workflows, your documentation, your revenue cycle. If governance isn't keeping pace, you're carrying more risk than you realize.
Healthcare organizations are moving fast on AI, and the efficiency gains are real. Faster clinical documentation. Automated prior authorizations. Predictive models that flag readmission risk before a patient leaves the floor. The tools work. The problem is that most organizations are deploying them without any governance structure in place, and that gap is where the liability lives.
Industry awareness of AI governance jumped from 40% to 70% in the last year. The sector knows it matters. What's lagging is execution.
What Governance Actually Looks Like in Practice
It's not a policy document that lives on a shared drive. AI governance is a set of operational systems: validation processes, audit trails, escalation protocols, and cross-functional accountability that govern how tools are deployed, monitored, and corrected over time.
Without it, you're deploying clinical AI faster than you can manage the exposure. Physicians distrust outputs they can't verify. Compliance teams can't produce audit trails when regulators ask. And when a model quietly degrades over time, there's no mechanism to catch it until something breaks.
Health systems that skip governance follow a predictable pattern: liability exposure, physician distrust, and eventually rolling back tools they spent months getting live, getting it right up front costs significantly less than unwinding it later.
Where Governance Breaks Down Most Often
Validation gaps. AI tools often get deployed after vendor demos and limited internal testing, without validation against your specific patient population, EHR environment, and care protocols. What performs well at an academic medical center may not perform as well at a community hospital.
No ongoing monitoring. Models drift. Patient populations shift. A tool that performed well at go-live can quietly degrade over months without anyone noticing until a clinical or billing error surfaces. Governance means building monitoring into operations, not treating deployment as the finish line.
Siloed ownership. When IT owns the tool, legal owns the risk, and clinical teams own the workflows, nobody actually owns governance. The organizations getting this right are building cross-functional steering with clear accountability and treating it as infrastructure.
Where to Start
You don't need a perfect framework before you move. You need a starting point: an inventory of the AI tools currently running in your organization, a clear owner for each one, and a basic set of monitoring criteria. From there, governance scales with your AI footprint.
If your organization is early in AI adoption, now is the right time to build the foundation. If you're already deep into deployment without a governance structure, the priority is a rapid assessment. Understand what's running, where the exposure is, and what needs immediate attention.
Safeguard Consulting Group works with healthcare organizations to build governance frameworks that are operational from day one. Whether you're starting from scratch or hardening an existing program, we help you move forward with confidence.
AI adoption in healthcare is not slowing down, and regulatory expectations around it are only going to increase. The organizations building governance now will have the least disruption when the scrutiny arrives. And it will.
Ready to assess your AI governance posture? Contact us at info@safeguardcg.com

The Hidden Risk Emerging Inside Healthcare Interoperability (Copy) (Copy)
Healthcare interoperability is transforming patient care, but it’s also exposing a growing governance challenge across the healthcare ecosystem. As organizations accelerate interoperability, APIs, AI platforms, and third-party integrations, the conversation is shifting from simply preventing cyberattacks to governing trusted access responsibly.
Healthcare has spent the last decade aggressively pursuing interoperability.
The goal makes complete sense: connected systems, faster access to patient information, improved coordination between providers and payers, and ultimately better patient outcomes.
But a recent report from The Washington Post highlights a growing issue healthcare leaders can no longer afford to overlook.
The concern is not a traditional ransomware attack or an external hacker breaking into hospital systems.
Instead, the issue appears to involve access occurring through the healthcare data-sharing ecosystem itself.
That distinction matters.
Modern healthcare environments are now deeply interconnected through EHR integrations, APIs, health information exchanges, digital health platforms, third-party applications, and AI-enabled workflows. Those connections are critical for operational efficiency and patient care, but they also create new governance challenges that many organizations are still learning how to manage.
Historically, healthcare cybersecurity conversations focused heavily on perimeter defense:
How do we stop attackers from getting in?
Today, the more difficult question may be:
Who already has access, and how well is that access governed?
As interoperability expands, healthcare organizations are increasingly dependent on external vendors, partners, applications, and downstream data relationships. In many cases, the operational risk is no longer coming from a direct breach. It comes from excessive permissions, weak oversight, fragmented identity management, or insufficient visibility into how sensitive data is being accessed and used.
This is where healthcare transformation becomes significantly more complex.
The industry cannot move backward on interoperability. Connected care is essential. AI initiatives, patient engagement platforms, analytics ecosystems, and coordinated care models all depend on trusted data exchange.
But modernization without governance creates exposure.
Healthcare organizations now need to think beyond simple compliance checklists and start treating governance as core operational infrastructure. Security, privacy, interoperability, and operational architecture can no longer operate as separate conversations.
The organizations that will lead the next phase of healthcare transformation will not simply be the most digitally advanced. They will be the ones capable of balancing innovation with operational discipline, visibility, accountability, and patient trust.
At Safeguard Consulting Group, we believe healthcare modernization must be approached with both execution and governance in mind. Technology acceleration is inevitable. The real differentiator will be how responsibly organizations scale it.

Healthcare Is Entering an Era of Forced Accountability
Healthcare is being forced into operational accountability. New regulatory pressure, rising cost scrutiny, and the expansion of AI are exposing gaps across payer systems, provider workflows, and data environments. Compliance is no longer about policy. It is about proving how systems actually perform under pressure.
Recent signals from both regulators and lawmakers are aligning in a way the industry can no longer ignore.
The proposed overhaul of the HIPAA Security Rule and the House Ways and Means Committee hearing with hospital CEOs are not isolated events. They are part of the same shift.
Healthcare is moving into a phase where systems must be explained, defended, and proven at an operational level.
Not in policy documents.
Not in executive summaries.
In the actual way systems function.
The End of “Policy-Level Compliance”
For years, healthcare organizations have been able to operate within a model where compliance lived in documentation.
Policies existed.
Controls were described.
Audits were periodic.
That model is breaking.
The proposed HIPAA changes introduce requirements that force organizations to demonstrate control at a system level:
Written and continuously updated asset inventories
Network maps that reflect real environments
More prescriptive risk analysis expectations
Stronger enforcement around access, encryption, and monitoring
This is not a documentation exercise.
It is an operational requirement.
Most organizations are not structured to meet it.
Cost Pressure Is Becoming Operational Scrutiny
At the same time, lawmakers are no longer accepting high-level explanations for rising healthcare costs.
During the Ways and Means hearing, hospital leadership was challenged directly on pricing, consolidation, and financial control.
This matters because cost pressure does not stay financial.
It moves downstream into operations.
Once pricing is questioned, the next layer is:
Revenue cycle integrity
Utilization management decisions
Contract configuration
Data consistency across systems
Vendor performance and cost contribution
Healthcare organizations are now being asked to justify outcomes that originate deep inside their systems.
AI Changes the Equation
The introduction of AI into healthcare operations accelerates everything.
AI does not rely on narrative.
It relies on data consistency, process clarity, and system behavior.
Once deployed at scale, AI exposes:
Workflow inefficiencies
Data mismatches across platforms
Delays in care and authorization
Variability in decision-making
Gaps between policy and execution
What was previously hidden inside system complexity becomes visible.
And once it is visible, it becomes measurable.
Then it becomes enforceable.
Interoperability Removes the Cover
Interoperability initiatives further compress the system.
Data is no longer confined to individual platforms.
It moves.
Across payers.
Across providers.
Across vendors.
This eliminates the ability to isolate problems within a single system.
If data does not reconcile, it is no longer a local issue.
It becomes systemic exposure.
The Real Problem: Systems Were Not Built for This
Most healthcare environments were designed to function, not to be interrogated.
They evolved over time:
Multiple payer platforms layered together
Provider systems operating independently
Vendor ecosystems expanding without full integration
Manual processes filling gaps between systems
These environments can operate day to day.
They struggle under scrutiny.
When asked to produce a clear, defensible view of how decisions are made, data flows, and outcomes are generated, they break.
What This Means for Healthcare Organizations
The shift underway is not incremental.
It changes the standard from:
“We are compliant.”
to
“We can prove how our system operates under pressure.”
That requires:
Full visibility into systems and data movement
Alignment between configuration, workflow, and policy
Control over vendor impact and dependencies
Operationalized compliance embedded into daily processes
The ability to explain and defend outcomes across the enterprise
This is not a project.
It is a restructuring of how systems are understood and managed.
Where Safeguard Operates
Safeguard Consulting Group works inside healthcare environments where this gap exists.
Across payer platforms, provider systems, and operational workflows, the focus is simple:
Bring systems under control so they can be understood, managed, and defended.
Not at a policy level.
At an execution level.
Because the next phase of healthcare will not be defined by who claims compliance.
It will be defined by who can prove it.

The Prior Authorization Reset: What AHIP’s Latest Move Signals for the Industry
Prior authorization is being rebuilt in real time. AHIP’s latest initiative signals a shift from manual control to automated, interoperable decision-making across healthcare.
The healthcare industry has reached a breaking point on prior authorization.
Long criticized for delaying care, increasing administrative burden, and frustrating both providers and patients, prior authorization is now undergoing one of the most coordinated reform efforts in recent history.
The latest announcement from America’s Health Insurance Plans marks a meaningful escalation in that effort.
What Just Happened
In its latest update, AHIP outlined the next phase of industry-wide commitments to streamline and simplify prior authorization across commercial, Medicare Advantage, and Medicaid managed care populations.
At its core, the initiative focuses on five structural changes:
Standardizing electronic prior authorization workflows
Reducing the number of services requiring prior authorization
Ensuring continuity of care during plan transitions
Improving transparency and communication on decisions
Expanding real-time approvals
The intent is clear: move prior authorization from a fragmented, manual process to a standardized, digital, near real-time system.
The Numbers Behind the Momentum
This is not just a policy announcement. Early execution is already underway.
Health plans have eliminated approximately 11% of prior authorization requirements, equating to millions fewer approvals required annually
The initiative impacts coverage affecting over 250 million Americans
The industry is targeting 80% real-time electronic approvals by 2027
At the same time, major payers are beginning to standardize submission requirements and digitize workflows at scale.
Why This Matters More Than It Looks
This is not incremental improvement. It is structural realignment.
Historically, prior authorization has been:
Manual
Inconsistent across payers
Highly administrative
Reactive rather than predictive
The AHIP initiative signals a transition toward:
Interoperability-first workflows (FHIR-based APIs)
Automation and real-time decisioning
Standardized clinical and administrative requirements
Reduced reliance on manual review processes
This is effectively the digitization of utilization management at scale.
The Strategic Implication: Control Is Shifting
The deeper implication is not operational. It is competitive.
For years, payers controlled friction through prior authorization. That friction acted as a gatekeeping mechanism for cost, utilization, and risk.
Now:
Standardization reduces payer differentiation in process
Automation reduces administrative leverage
Transparency increases accountability
The battleground is shifting away from control of approvals toward:
Clinical value
provider experience
workflow integration
speed of decision-making
In short: prior authorization is moving from a control tool to a service layer.
The Reality Check
Despite progress, skepticism remains.
Physicians still report high administrative burden, averaging dozens of prior authorization requests weekly.
And key gaps remain:
Prescription drug prior authorization is not fully addressed
Provider adoption of new digital workflows is uneven
Interoperability execution is still early-stage
This means the industry is in transition, not resolution.
What Healthcare Leaders Should Be Watching
This shift creates immediate implications across the ecosystem.
Health Plans
Must modernize UM infrastructure rapidly
Need to operationalize FHIR-based workflows
Risk falling behind if execution lags commitments
Providers
Will benefit from reduced friction
But must invest in digital integration to realize gains
Health Tech & Services Companies (Safeguard positioning)
Massive opportunity in:
workflow optimization
API integration
prior auth automation
data standardization
The Bottom Line
AHIP’s latest move is not just about simplifying prior authorization.
It is about redefining how care access decisions are made, processed, and experienced.
The winners in this next phase will not be those who reduce prior authorization the fastest.
They will be the ones who rebuild the system around speed, transparency, and seamless workflow integration.

Rural Hospitals Have a Narrow Window to Use the New $50 Billion Federal Fund Wisely
Rural hospitals are operating under sustained pressure, with rising costs, workforce shortages, and nearly 200 closures over the past two decades. The new $50 billion federal Rural Health Transformation Program creates a rare opportunity, but the funding is temporary while the challenges are not. The organizations that use this moment to strengthen EHR strategy, improve interoperability, and build connected care models will create lasting stability. Those that treat it as short-term relief will face the same constraints once the funding runs out.
Rural hospitals are under pressure from every direction: tighter margins, workforce shortages, administrative burden, and rising costs. The urgency is not theoretical. The UNC Sheps Center reports 195 rural hospital closures or conversions since January 2005, including 152 since 2010. Separately, the American Hospital Association cited Sheps data showing that proposed federal cuts in 2025 could place more than 300 rural hospitals at risk of closure, conversion, or service reductions. The AHA’s 2026 cost report also found that hospital expenses grew 7.5% in 2025, with workforce costs up 5.6%, supplies up 9.9%, and drug costs up 13.6%.
That is the backdrop for the federal Rural Health Transformation Program, the new $50 billion rural health fund administered by CMS. The program makes $10 billion available each year from fiscal 2026 through fiscal 2030. CMS states that 50% of each year’s funding is distributed equally among approved states, while the other 50% is allocated based on factors such as rural population, rural facilities, and hospital conditions in the state. CMS announced first-year awards to all 50 states on December 29, 2025, with 2026 awards averaging about $200 million per state.
This matters, but the structure of the fund matters even more. KFF notes that the money is temporary, while many of the underlying financial pressures are not. The law provides funding only through 2030, funds must generally be spent by the end of the following fiscal year, and all funds must be spent before October 1, 2032. KFF also notes that the fund was created against a backdrop of much larger projected Medicaid reductions, meaning the rural fund can help stabilize and modernize systems, but it is not a permanent operating backstop.
The practical implication is simple. Rural organizations should not treat this as bailout money. CMS explicitly frames the program around sustainable transformation. The program allows states to fund training and technical assistance for technology-enabled solutions, software and hardware for major IT advances, cybersecurity capability development, technology-driven chronic disease tools, and coordination models that let rural facilities share operations, technology, primary care, specialty care, and emergency services. CMS also says states should prioritize long-term improvements rather than perpetual operating expenses.
That is where EHR strategy becomes central. CMS specifically says upgrades, enhancements, added modules, interfaces, and new functionality for existing EMR or EHR systems are allowable uses of funds and are not subject to the program’s 5% limitation. The 5% limit applies to replacing an existing certified EMR with a completely new one. CMS also says those upgrades should align with CMS and ASTP/ONC interoperability criteria. In other words, rural hospitals do not have to choose between doing nothing and ripping everything out. They can use the fund to strengthen what they already have, connect it better, or selectively move toward a more scalable model.
That makes shared and managed EHR models highly relevant. Epic says health systems have used Community Connect since 2007 to extend their Epic instances to nearby medical groups, allowing them to gain access to Epic without hiring internal support teams or purchasing infrastructure. Epic also says more than 1,000 hospitals and 22,000 clinics using Epic are now live on TEFCA through Epic Nexus, underscoring the growing importance of networked interoperability. Outside Epic, Oracle positions CommunityWorks as a fully managed model for community, rural, and critical access hospitals, and MEDITECH positions MaaS as a cloud-based model that gives smaller organizations enterprise-level tools without major capital investment or on-premise infrastructure.
The case for these models is not just vendor marketing. ASTP’s 2023 hospital interoperability brief found that only 36% of rural hospitals were routinely interoperable, compared with 47% of urban hospitals. It also found that only 22% of independent hospitals were routinely interoperable, versus 53% of system-affiliated hospitals. More broadly, 71% of hospitals said necessary outside clinical information was routinely available at the point of care, but only 42% said clinicians routinely used it when treating patients. That gap is exactly where better implementation, cleaner interfaces, stronger governance, and smarter workflow design matter.
The fund’s rules also make clear what disciplined execution looks like. Broadband infrastructure is not an allowable use of funds. New construction is not allowed. Minor alterations and renovations are capped at 20% of the total award in the childcare example CMS gives. Provider payments are capped at 15% of a state’s award for that category and must tie to specific transformation initiatives and outcomes. CMS has already appropriated the full $50 billion, but it expects states to avoid duplication, avoid supplanting existing funding, and build plans that survive after the federal money ends.
So the real opportunity is not “buy software.” It is to build a rural health operating model that can last after the grant period. For some organizations, that will mean Epic Community Connect. For others, it will mean optimizing an existing platform, adding interoperability layers, tightening cybersecurity, improving referral and transfer workflows, enabling telehealth or remote monitoring, or moving to a managed platform better suited to a rural cost structure. The wrong move is chasing a large technology purchase without a sustainable operating model behind it. The right move is using this funding window to reduce fragmentation, strengthen local access, and create an implementation plan that a rural organization can actually support five years from now.
That is the opening for experienced execution support. Rural hospitals and health systems do not just need strategy decks. They need help evaluating whether to stay, optimize, connect, or migrate. They need program governance, vendor selection discipline, interface planning, legacy data strategy, implementation management, workflow redesign, and change management that fits the realities of rural operations. This is the kind of work Safeguard Consulting Group can support: practical, execution-focused help for rural health initiatives involving Epic Community Connect, interoperability modernization, and right-sized EHR strategies for smaller systems.
The $50 billion rural health fund is real. The window is finite. Rural organizations that turn it into durable operational and clinical improvement will be in a far stronger position than those that treat it like temporary relief

The Coding Game Is Over. Most Payers Haven’t Realized It Yet.
For years, payer growth was driven by how well risk was documented, not how well it was managed. That model is breaking. As pressure builds from regulators, rising costs, and outcomes, coding is no longer the strategy, it is the baseline. The real shift is underway, and it forces a harder question: can payers move beyond capturing risk and actually change it?
For years, payers found a reliable way to grow.
Document more.
Code better.
Capture more risk.
It worked so well that entire operating models were built around it. Vendors scaled. Teams expanded. Technology followed.
Revenue didn’t just come from managing health.
It came from how well you described it.
That model is now breaking.
And most organizations are still playing by the old rules.
What’s changed isn’t subtle.
Oversight on risk adjustment is tightening.
Payment pressure is increasing.
Medical costs are accelerating faster than premium growth.
The result is simple.
You can’t code your way to growth anymore.
This is where the disconnect starts.
Most payer organizations are still optimized for documentation, not outcomes.
They are built around:
Retrospective chart reviews
Coding audits and vendor programs
Documentation capture strategies
All of it designed to make sure nothing is missed.
But nothing about that model actually improves the health of a member.
It just improves how the condition is recorded.
That distinction didn’t matter as much before.
Now it does.
Because growth is shifting.
Not from how well you capture risk.
But from how well you manage it.
And that’s a completely different capability.
It requires identifying risk earlier.
Intervening in real time.
Closing care gaps before they turn into cost.
That’s not a coding function.
That’s operational execution.
Here’s the problem.
You can’t take a system designed to look backward
and expect it to perform looking forward.
The workflows don’t match.
The incentives don’t align.
The infrastructure isn’t there.
And yet, many plans are still trying to stretch documentation engines into clinical ones.
At the same time, the economics are shifting underneath them.
The return on coding optimization is shrinking.
The cost of poor outcomes is rising.
Avoidable admissions.
Chronic disease mismanagement.
Member churn tied to experience.
These aren’t side issues anymore.
They are margin drivers.
This is the part most organizations are underestimating.
Coding is no longer the strategy.
It’s the baseline.
Everyone is expected to get it right.
No one is going to win because of it.
The winners will be the plans that move first.
The ones that shift from retrospective capture
to proactive intervention.
The ones that stop asking, “Did we document it?”
and start asking, “Did we change it?”
Most payer organizations won’t make this shift quickly.
Not because they don’t understand it.
But because their entire operating model is built for something else.
And that’s where the opportunity sits.
The coding game isn’t evolving.
It’s ending.
The only question is how long it takes before your organization realizes it.

Why Healthcare Providers Are Spending Billions Just to Get Paid
Providers are spending over $25 billion a year just to get paid, not because claims are wrong, but because the system slows down valid ones. Most denied claims are eventually approved, exposing a costly cycle of rework, delays, and unnecessary administrative burden.
Getting paid in healthcare should be simple.
It isn’t.
Providers are now spending over $25 billion a year just working through claims. Not because the claims are wrong, but because the process is.
About 15% of claims get denied upfront. That sounds reasonable until you realize most of them are eventually approved and paid anyway.
That means the system is not catching bad claims. It is slowing down good ones.
Every denial triggers the same loop. Review. Resubmit. Wait. Repeat. Weeks turn into months. Multiply that across thousands of claims and the cost explodes.
This is not a technology issue. It is a workflow problem built into the system itself.
Then there is prior authorization. Providers ask for approval before care. They get it. Then the claim can still be denied later.
So now they ask for permission, receive permission, and still have to fight to get paid.
That is not control. That is duplication.
The impact is immediate. Hospitals are operating with tighter margins than they have in years. Cash is delayed. Staff is tied up in administrative work. Investment in care gets pushed out.
At the same time, these inefficiencies drive up costs across the system, contributing to higher premiums.
Nothing about this is accidental. The system is doing exactly what it was built to do.
The problem is what it was built to do no longer makes sense.
Most denied claims end up getting paid. Billions are spent proving what was already true.
Until payer rules are standardized, unnecessary approvals are reduced, and claims are validated before submission, this does not change.
Providers will keep funding a process that works against them.
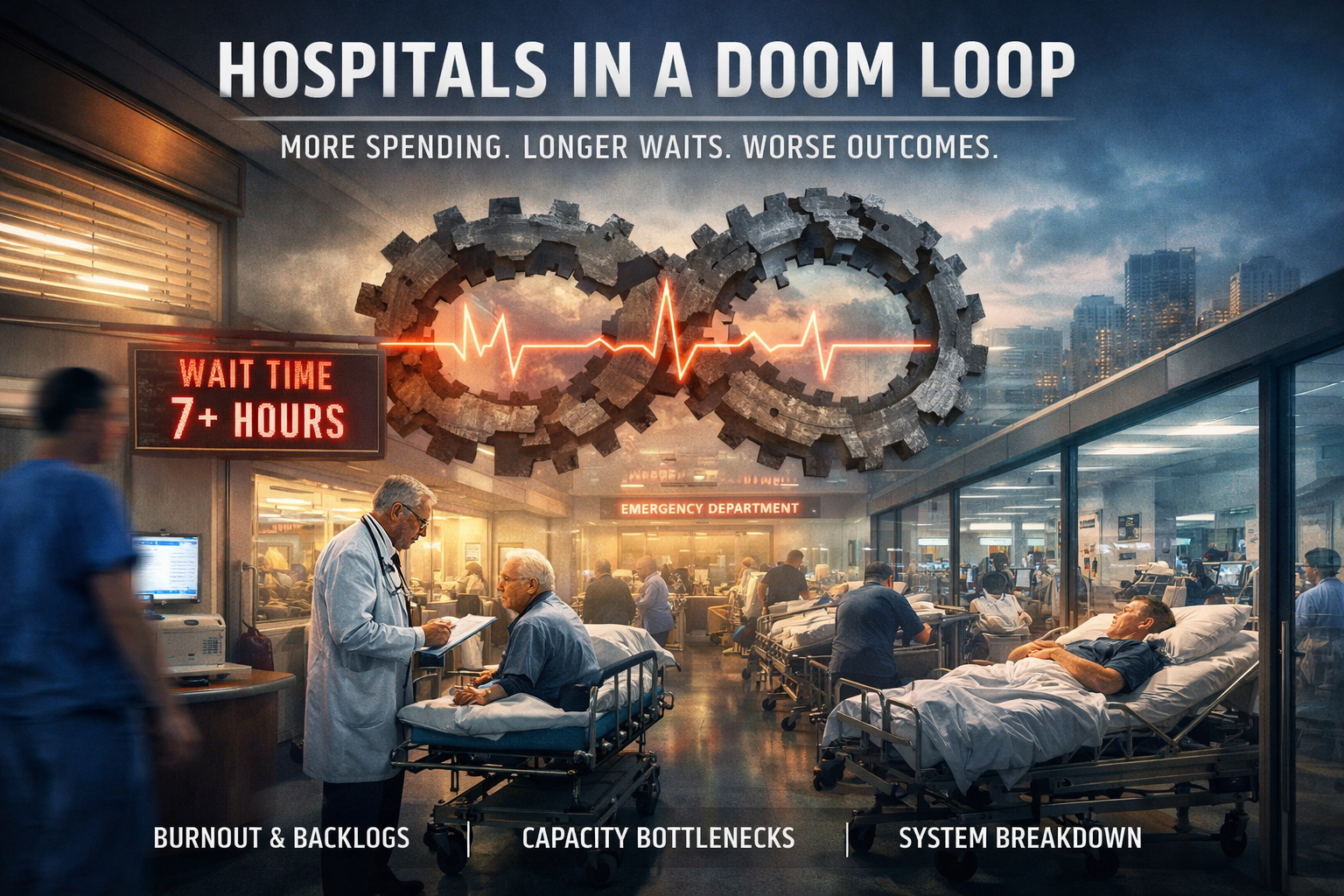
Hospitals in a Doom Loop: Why Healthcare Is Slowing Down as Spending Rises
Hospitals are spending more and staffing more, yet moving patients slower than ever. The issue isn’t resources. It’s broken flow. As delays compound and patient complexity rises, healthcare systems are trapped in a self-reinforcing loop that funding alone can’t fix.
Hospitals are doing more than ever and getting less done.
Spending is up. Staffing levels have increased. Technology investment has never been higher. Yet patients are waiting longer, outcomes are slipping, and frontline staff feel like they are moving slower, not faster.
A recent analysis from The Economist puts a name to what many operators already know: hospitals are stuck in a self-reinforcing loop that is degrading performance instead of improving it.
The Shift No One Reversed
The healthcare system did not recover from the pandemic. It adapted to dysfunction.
During COVID, hospitals were forced into reactive mode. Elective procedures stopped. Throughput collapsed. Backlogs built. Staff stretched beyond sustainable limits.
That was expected.
What wasn’t expected is that the system never returned to baseline. The temporary state became permanent.
Patients came back sicker. Staffing came back less experienced. Processes came back slower.
And the system locked into a new equilibrium.
A worse one.
The Loop That Is Breaking Hospitals
The problem is not isolated. It compounds.
Patients wait longer to be seen.
Longer waits mean more advanced illness.
More advanced illness requires longer, more complex care.
Longer care blocks beds and staff.
Blocked capacity increases wait times again.
This is not congestion. It is a feedback loop.
Hospitals are no longer dealing with volume spikes. They are operating inside a system that continuously manufactures delay.
Why More Money Made It Worse
The instinctive response has been to add resources.
More staff. More funding. More capacity.
But output has not followed.
Because healthcare is no longer constrained by inputs. It is constrained by flow.
Adding staff into a slowed system does not increase throughput. It often reduces it. Newer clinicians require more coordination. Decision-making slows. Variability increases.
At the same time, every patient now consumes more time.
Deferred care during the pandemic created a wave of higher-acuity cases. Chronic illness is rising. Aging populations are increasing demand intensity, not just demand volume.
So even as staffing numbers rise, effective capacity falls.
More people. Less movement.
The Flow Problem No One Owns
Hospitals are not failing on the inside. They are failing at the edges.
A patient who cannot access primary care shows up in the emergency department.
A patient who cannot be discharged stays in a hospital bed.
A patient who needs post-acute care waits because no placement exists.
Every breakdown outside the hospital becomes a bottleneck inside it.
Beds turn into holding areas. Emergency departments turn into queues. Clinicians spend time managing movement instead of delivering care.
What looks like a hospital problem is actually a system problem.
But no one owns the system.
Technology Didn’t Solve It
The industry invested billions into platforms like Epic and Cerner.
Data is everywhere.
But movement is not.
Most systems were built to document care, not accelerate it. They capture information but do not coordinate action in real time. They add visibility without removing friction.
The result is a paradox.
More data. Slower decisions. Lower throughput.
What This Actually Means
Healthcare is not collapsing from lack of investment.
It is stalling from lack of coordination.
Until systems are redesigned around flow, nothing else scales. Not staffing. Not funding. Not technology.
The organizations that break this loop will not be the ones that spend more.
They will be the ones that move faster.
Because in the current environment, speed is capacity.
And right now, capacity is the one thing healthcare no longer controls.

AI in Payer Operations: Efficiency Tool or Legal Liability?
AI is rapidly becoming embedded in core payer operations, driving decisions across claims, prior authorization, and risk adjustment. But as automation increases, so does exposure. The real challenge isn’t adoption—it’s accountability. As AI begins to influence outcomes at scale, payers must confront a critical question: can they explain and defend the decisions their systems are making?
The payer industry is moving fast on AI.
Claims are being automated. Prior authorizations are being streamlined. Risk adjustment is being augmented. Call centers are being replaced with conversational models.
The story everyone is telling is simple.
AI drives efficiency. Efficiency drives margin.
That story is incomplete.
What’s actually happening is this:
AI is moving faster than the controls required to manage it.
And that gap is where the real risk sits.
AI is no longer a support tool. It’s embedded directly into decision-making.
It determines whether a claim is paid.
It influences whether a prior authorization is approved.
It flags what gets reviewed and what gets ignored.
That shift matters.
Because once AI starts making decisions, you’re no longer optimizing workflows.
You’re automating judgment.
And most organizations are not set up to govern that.
There’s a problem building under the surface that few teams are willing to say out loud.
First, accountability starts to break down.
When a decision is driven by an algorithm, ownership becomes unclear.
Was it the plan? The vendor? The model?
In a manual process, responsibility is obvious.
In an automated one, it fragments.
Second, explainability becomes a real issue.
It’s easy to say a model flagged something.
It’s much harder to explain why in a way that stands up to audit, appeal, or legal review.
If you can’t clearly defend a decision, the efficiency you gained becomes irrelevant.
Third, and most important, mistakes scale.
A human makes errors one at a time.
AI makes them thousands at a time.
If the logic is flawed, the impact isn’t contained. It compounds quickly and quietly.
By the time it’s discovered, the exposure is already material.
This is where the industry is headed.
AI-driven decisions are starting to attract scrutiny.
Litigation is emerging.
Regulators are behind, but not indefinitely.
The imbalance is obvious.
Decision velocity is increasing. Oversight is not.
That doesn’t hold for long.
The mistake most payers are making is treating AI like a technology upgrade.
It gets handed to IT.
It gets implemented through a vendor.
It gets measured in terms of cost reduction.
That framing misses the point entirely.
AI in payer operations is not just a technology layer.
It is a decision layer.
And decision layers require control, accountability, and governance.
Right now, many organizations don’t have that foundation in place.
What needs to change is straightforward, but not easy.
Every automated decision needs to be traceable.
Every outcome needs to be explainable.
Every workflow needs to be defensible.
Not in theory. In practice.
Human oversight isn’t going away in high-risk areas.
It just needs to be redesigned around the system, not bolted on after the fact.
AI will continue to expand across payer operations. That’s not the question.
The real divide will be between organizations that deploy it
and organizations that can defend it.
Because the next wave of pressure won’t come from innovation.
It will come from scrutiny.
The question is no longer whether to use AI.
It’s whether your organization can stand behind the decisions it makes when AI is involved.

The White House Built a “News App.” It Looks a Lot Like Surveillance
This “White House news app” wants your location, your biometrics, and control over your device. That’s not a feed. That’s something else.
The White House recently launched a mobile app described as a direct, unfiltered news feed. On the surface, that sounds like a simple modernization of communication—cut out the middleman, deliver information straight to the public, and control the narrative without distortion.
But that framing breaks down the moment you examine how the app actually behaves.
This is not just a content platform. It is a government-operated application with system-level access to personal devices, and that changes the conversation entirely.
A typical news app has a narrow purpose. It delivers articles, videos, and notifications. It does not need to know where you are, who you are beyond a login, or what else exists on your device. It certainly does not require biometric identifiers or the ability to control how your device operates in the background.
This app does.
The permissions tell the real story. Ignore the branding and look at what the application actually requests: precise location access, full network connection visibility, biometric and fingerprint authentication, the ability to prevent the device from sleeping, and permission to modify or delete contents in shared storage.
A standard news app does not need this level of access.
Each of these permissions can be explained away in isolation. Together, they form something very different. They enable continuous location awareness, persistent background activity, identity-level linkage, and access to user-stored data. That combination is not about improving a user experience. It is about establishing infrastructure-level control.
The more important issue is not just what the app can access, but what happens after that access is granted. There is limited transparency around how data is collected, how frequently it is transmitted, whether it is shared with third parties, and how long it is retained. In any other context—particularly one involving sensitive systems—this lack of clarity would immediately trigger scrutiny.
That’s where the healthcare IT lens becomes useful.
In healthcare, systems are built around strict principles of data minimization, explicit consent, and traceability. Under HIPAA, organizations are required to justify every piece of data they collect, define exactly how it is used, and maintain auditable controls over access and retention. An application requesting this level of access without clear disclosure would not pass a compliance review. It would be flagged as a risk.
Outside of healthcare, those standards are not consistently applied. Consumer applications—and increasingly, government-facing platforms—operate in a gray area where capability often outpaces governance. That gap is where concern should live.
Because when you combine a direct government communication channel with deep device-level permissions and unclear data practices, the result is not just a better way to distribute information. It is the foundation for something much broader: the ability to link identity, behavior, and environment in a continuous and largely invisible way.
This is why comparisons to Big Brother continue to surface. Not because of rhetoric, but because of structure. A centralized authority controlling its own messaging, operating through devices people carry at all times, with the technical capability to observe and collect data at scale.
The difference is that this model is not imposed. It is adopted. Users download the app, grant permissions, and carry it with them voluntarily. That makes it more efficient, more scalable, and far less visible than anything imagined in Nineteen Eighty-Four.
If this were just a news app, it would behave like one.
It doesn’t.
At a certain point, the distinction between communication and surveillance stops being theoretical. It becomes architectural.
And once that shift happens, the warning is no longer metaphor.
Big Brother is watching.

Infosys Acquires Optimum Healthcare IT: Healthcare Transformation Is Being Consolidated
Infosys’ acquisition of Optimum Healthcare IT signals a fundamental shift in healthcare transformation. The industry is moving away from specialized consulting firms toward large, integrated platforms that control strategy, implementation, and long-term operations. For healthcare organizations, the real risk is not capability but control. As consolidation accelerates, choosing the right partner will determine who owns your roadmap, your data, and ultimately your future.
The acquisition of Optimum Healthcare IT by Infosys is not just another services deal. It is a clear signal that healthcare transformation is no longer driven by niche expertise. It is being consolidated by global platforms.
If you are a healthcare executive, this directly impacts how you choose partners, how your systems evolve, and how much control you retain over your transformation.
Scale Is Replacing Specialization
For years, firms like Optimum Healthcare IT built their reputation on deep provider-focused expertise, especially in EHR implementation, optimization, and large-scale system transformation.
That model is now being absorbed.
Infosys is not acquiring Optimum to preserve a boutique consulting approach. It is acquiring it to industrialize that expertise and plug it into a global delivery engine powered by AI, automation, and offshore scale.
This changes the value proposition.
Healthcare organizations are no longer buying expertise alone. They are being sold platforms, delivery models, and long-term dependency on a single ecosystem.
This Is About Control, Not Capability
On the surface, this looks like a win for healthcare providers:
Broader capabilities
End-to-end transformation services
Access to global innovation and AI
But the dynamic shifts underneath.
When transformation is owned by large integrated firms:
Control moves away from the provider
Flexibility decreases
Standardization increases, whether it fits your organization or not
As consolidation increases, the number of truly independent advisors shrinks.
The End of Fragmented Vendors
Healthcare organizations used to assemble their own ecosystem:
One firm for advisory
Another for implementation
Another for optimization
That model is disappearing.
Large firms like Infosys are building closed-loop service models:
Strategy to implementation to managed services to optimization, then repeat.
Once you enter that loop, exiting becomes difficult. This is intentional.
AI Is the Justification, Not the Strategy
Every acquisition today is framed around AI, cloud, and automation.
Those drivers are real, but they are not the core strategy.
The strategy is consolidation.
AI makes consolidation easier to justify and easier to sell.
By combining Optimum’s provider expertise with its own AI and cloud platforms, Infosys strengthens its position as a single-source partner. The real question for healthcare organizations is whether they are adopting AI to improve operations or to fit into a vendor-controlled platform.
What Healthcare Leaders Should Be Asking
Most organizations will evaluate this type of acquisition at a surface level. That is a mistake.
The real questions are:
Who owns your transformation roadmap, your team or your vendor
How easily can you switch partners once you are embedded in a global delivery model
Are you buying outcomes or committing to long-term dependency
This shift creates dependency at scale.
The Market Is Moving Toward Fewer, Larger Players
This deal is part of a broader pattern. The healthcare IT services market is consolidating around a small number of global firms that offer:
Deep vertical expertise
Scalable delivery models
Integrated technology platforms
This combination is powerful, but it reduces choice.
As consolidation accelerates, healthcare organizations will face fewer alternatives, less negotiating leverage, and increased exposure to vendor-driven strategies.
Where This Leaves You
If you are leading digital transformation in a healthcare organization, the takeaway is direct.
Stop evaluating vendors based only on capability. Start evaluating them based on control.
Capability is now expected.
The real differentiators are:
Who owns the data
Who controls the roadmap
Who dictates the pace of change
Infosys acquiring Optimum Healthcare IT is not just another transaction. It marks a shift.
Healthcare transformation is being centralized, standardized, and scaled.
If you are not actively managing that shift, you are being absorbed by it.
Epic, Microsoft collaboration will bring AI technology to healthcare
OpenAI drafts messages for providers with the goal of reducing administrative burdens.
Three organizations are currently live with the Azure OpenAI message drafting software: UC San Diego Health, UW Health, and Stanford Health Care.
Thanks to a collaboration between Epic Systems and Microsoft, healthcare providers can now receive a time-saving hand from generative AI technology that drafts responses to patient messages and inquiries.
For years, Microsoft has allowed Epic to use the cloud hosting platform Azure as part of their longstanding collaboration, Garrett Adams, product lead for Epic’s Ambulatory Research and Development Division and member of the Cognitive Computing Platform team, said.
The recent expansion involves the use of Azure OpenAI, which Adams described as a large language model that is “very good at predicting the next word.” This specific technology has been trained over a large collection of information to draft responses to patient messages for providers.
“It is really a master of language,” Adams said.
Utilizing OpenAI will save an incremental amount of time for the provider to respond to patients, Adams said. This became especially relevant after the pandemic, which saw a large rise in telehealth services and patient messaging.
The asynchronous messaging model happened to prove itself so useful during the pandemic that it stuck around, Adams said. The goal now is to reduce the workload associated with responding to such messages.
“This overall has incredible potential in our industry to reduce the administrative burden, to automate mundane tasks and to give providers as much as that face-to-face time with patients as possible,” he said.
By using the Azure OpenAI service, Epic can leverage patient data and information securely because it is HIPAA compliant, Adams said.
Adams emphasized the AI technology provides draft messages, meaning the messages are not automatically sent. Healthcare providers can review the AI generated message, modify and then send it – or opt to draft a blank message as they would’ve before.
An example of the technology is when patients reach out to providers for information about medication refills. The AI brings in additional information from the chart in a secure, private way and combines that data with the patient request – along with some additional cues for sentence structure and tone to avoid sounding robotic, Adams said.
Generative AI is also being used in Epic’s reporting tool SlicerDicer to enhance conversational support, Adams said. Through SlicerDicer, providers can customize searches and find data on patient populations.
Prior to this technology, providers had to filter through information and hunt through directories but can now have a time-saving conversation with the software for information via chat or voice, Adams said.
“I think that as much as we can do to improve the happiness and reduce the burden on users – that’s just gonna pay dividends on the care that they’re able to provide for patients,” he said.
Three organizations are currently live with the Azure OpenAI message drafting software: UC San Diego Health, UW Health and Stanford Health Care. These organizations are experimenting with a subset of users that Epic has helped set up for success, Adams said.
“We’re taking a very thoughtful and incremental approach to how we roll this out,” he said.

CMS Taking Steps to Modernize Approach to Digital Technologies
May 03, 2019 - CMS is working with other federal agencies and lawmakers in Congress to modernize its approach to coverage for data-driven medical devices and other innovative technologies.
As digital tools, companion apps, and analytics technologies become more commonplace across the industry, CMS hopes to speed up the process of determining payment rates for breakthrough advances in patient care, CMS Administrator Seema Verma said in a speech at the Medical Device Manufacturers Association Annual Meeting this week.
“Our vision is ambitious yet achievable: to protect and secure Medicare and ensure beneficiaries have access to the latest medical technologies,” said Verma.
“The advent of novel medical technologies requires CMS to remove barriers to ensure safe and effective treatments are readily accessible to beneficiaries without delaying patient care. In essence, keeping new technologies and treatments moving from bench to bedside—and into the hands of those who need them most.”
CMS is anticipating the continued development of medical devices and other products that incorporate advanced analytics, data interoperability, and machine learning to offer actionable insights for patients and providers at the point of care.
Integrating new products and services into the Medicare fee schedule can be a lengthy and complex process, however, said Verma.
CMS and its Medicare Administrative Contractors (MACs) must first make coverage decisions on a national or local level. Then the agency must determine if the new technology can be coded for payment with existing codes or if new codes are needed.
Lastly, the agency makes a payment determination, taking into account the site and purpose of use in addition to other criteria.
Medicare can take years to make these decisions. Oftentimes, coverage for a “new” technology or device can lag behind commercial coverage by as much as a decade.
As the pace of innovation accelerates as the healthcare industry enters the age of artificial intelligence, this snail’s pace is simply no longer acceptable, said Verma, especially as other agencies such as the FDA take proactive steps to modernize their processes.
“With the remarkable number of transformative technologies coming to market — many with unprecedented price tags — Medicare must develop new frameworks that will support tomorrow’s innovations and endure the test of time,” she said.
“Simply put, our goal is to get new innovations to our beneficiaries concurrent with FDA approval by removing government barriers to innovation and harmonizing CMS coverage, coding, and payment processes.”
CMS has proposed several changes to payment policies for medical devices that receive “breakthrough device” designations from the FDA.
“This includes waiving the requirement for ‘substantial clinical improvement,’ which is one of the criteria that must be met for CMS to make additional payments,” said Verma. “For devices granted Breakthrough-designated FDA approval, real-world data regarding outcomes in different patient populations is often limited at the time of approval, making it hard for innovators to meet this requirement.”
“Waiving this requirement would provide additional Medicare payment for the technologies for a period of time while real-world evidence is emerging, so Medicare beneficiaries don’t have to wait for access to the latest innovations.”
Medical devices on the market for two years would still have to demonstrate substantial clinical improvement to qualify for a third year of payment, but putting products into the market more quickly will allow patients to benefit from innovations immediately, she added.
By collaborating more closely with the FDA, CMS is repositioning Medicare as an innovation leader instead of a barrier to bringing new devices and technologies to some of the nation’s neediest patients.
“We are also working with Congress on a raft of legislative changes to address the challenges we face in adapting the Medicare program to modern technology,” Verma continued. “For example, the President’s Budget proposes expanding coverage of disposable devices, such as innovative glucose monitors and insulin pumps that substitute for a durable device, for use in the management and treatment of diabetes.”
“If we implement all of these changes, we will ensure beneficiaries have access to the latest technologies in a timely manner; improve the innovator experience with Medicare; create predictable coverage pathways; enhance opportunities for coverage for transformative technologies; reduce wait times for permanent codes; and modernize payment for innovative services.”
These efforts align with Verma’s signature Patients Over Paperwork initiative, which aims to reduce unnecessary complexity for beneficiaries and providers.
“Patients over Paperwork is an agency-wide effort to solicit input from stakeholders on policies that are outdated, redundant, or overly burdensome, and to make updates in response,” she explained.
“We believe these changes clarify and simplify the process, helping to ensure that manufacturers get appropriate therapies and medical devices to patients more efficiently. These improvements respond to stakeholders’ suggestions for more transparency, including multiple opportunities for engagement with CMS and our MACs.”
Making widespread changes to such a large and influential government entity isn’t easy, Verma acknowledged, but collaborating with industry stakeholders and other agencies will help to advance the adoption of cutting-edge analytics and innovative medical devices in a safe and effective manner, she concluded.
“A modernized CMS, with stronger inter-agency collaborations with FDA and NIH, will unleash innovation for years to come, and be a catalyst for improving quality, enhancing access, increasing efficiency, and lowering costs.”

Faulkner Guides Epic Systems from EHR to Comprehensive Health Record
At HIMSS18, Epic Systems founder and CEO Judy Faulkner shared her vision for a comprehensive health record and continued improvements to interoperability.
Epic Systems founder and CEO Judy Faulkner has a reputation for big ideas.
And with some of the top health systems in the country among her customers and around two-thirds of patients owning a current Epic record, the company and its leader tend to have their sites set at scale.
Faulkner has dedicated decades to growing her company into a market mover that features prominently in any discussion of the health IT space, and her yearly presence at the annual HIMSS Conference and Exhibition punctuates how serious she is about bringing her big ideas not just to her own clients, but to the healthcare system at large.
Judy Faulkner, Founder and CEO of Epic Systems
Source: Epic Systems
Moving from paper charts to electronic health records has been a difficult enough leap for many, but Faulkner believes that her community of customers is ready for the next big shift in thinking: stepping up from the EHR to the CHR.
The “E” has become irrelevant, she asserted, reinforcing an idea that is guiding Epic towards increased interoperability, simplified workflows, and more open communication between disparate organizations.
It’s time to stop dwelling on the difference between paper and processing power and start reexamining how patient records look, feel, and function in the era of data-driven insights and value-based care, she stated.
“Saying ‘electronic health record’ is like saying you have an electronic iPhone,” Faulkner told HealthITAnalytics.com. “It’s no longer a meaningful distinction for the industry now that almost everyone is off of paper.”
“The comprehensive health record goes way beyond the 10 percent of care that physicians and hospitals directly contribute. It incorporates genomics, environmental data, family history, socioeconomics – all of the factors providers will be responsible for as they stop getting paid for the 10 percent and start earning money based on keeping the patient whole.”
USING THE PATIENT RECORD TO ADDRESS THE SOCIAL DETERMINANTS OF HEALTH
The social determinants of health are top of mind for Faulkner, who has shifted away from playing defense and instead has started to strike a much more forward-looking tone.
“The social determinants have been largely missing from healthcare,” she said. “Understanding that loneliness, for example, has a 70 percent overlap with morbidity can change the way we look at individuals and what they need.”
“We’re going to try to use the tools we have to assess who we can help by creating a friendlier environment, especially for older people who might have lost their spouse, or don’t have any support system, or might not be able to cook for themselves or drive.”
Using health IT to better understand individuals and help patients overcome their personal challenges, such as smoking, will allow providers to see more success under value-based contracts, said Faulkner.
“Saying ‘electronic health record’ is like saying you have an electronic iPhone. It's no longer a meaningful distinction."
Achieving that goal will require vendors to extend their systems into places where they have not yet secured a foothold, she added.
“We need to help the patient understand which of their personal behaviors are not helping them. Our systems are even now being extended into those areas to bring data back and advice to the patient to make our care of them much more complete.”
Bringing the care continuum closer together through better data exchange is crucial for succeeding with population health initiatives, whether they are risk-based or not.
“When you bring a system like Epic into some of the places we need to be, such as a behavioral health program, you can allow those providers to add to the existing comprehensive record instead of creating new, fragmented records of care at different places,” she explained.
“Then you can share that information with providers at the patient’s care hub, whether that’s a hospital or a primary care provider. Interoperability is the key to that.”
“WE COULD JUST WAIT, OR WE COULD DO SOMETHING”
Epic Systems hasn’t always enjoyed the best reputation when it comes to interoperability, and Faulkner has been keenly aware of that fact.
The company has endured some bruising PR body blows from competitors and lawmakers who have taken exception to Faulkner’s approach to sharing data.
The use of terms like “data blocking” has often been seen as a veiled reference to Epic’s exclusivity. Creating a closed community centered entirely on one vendor’s customers, no matter how seamlessly it could exchange data internally, is the opposite of meaningful interoperability, many stakeholders have argued.
Unsurprisingly, Faulkner vehemently disagrees.
“I know there are people who say that Epic is only focused on Epic. But when we first built the system in the early 2000s, well before meaningful use, we had to invent the whole thing,” she said.
“At the time, I talked to some people at HIMSS and asked if they were going to standardize the data so we could – I don’t think I even knew the word ‘interoperability’ yet – but I wanted to know if we could create some standards to exchange the data back and forth. The folks at HIMSS said we shouldn’t hold our breath.”
Epic had two choices, she continued. “We could just wait, or we could do something. We decided to do something.”
That “something” has evolved into a multifaceted platform that integrates a core EHR with patient-provided data, big data analytics, health information exchange capabilities, and integrated workflows allowing access to data from both internal and external customers.
“Just because there’s no standardization doesn’t mean we shouldn’t go ahead anyway,” said Faulkner.
“If we at least start doing what we can with what we have, it’s going to help millions of patients who are cared for using our software. Then other people can see it and join in when there are standards, and we will be more than happy to work alongside them, too.”
"I wanted to know if we could create some standards to exchange the data back and forth. The folks at HIMSS said we shouldn’t hold our breath.”
The Epic strategy has coalesced around three key components that contribute to creating the comprehensive health record.
“We’re treating everything as one system,” said Faulkner. “It’s the first step towards making one unified record for every patient. That’s what everyone has talked about, albeit in different ways.”
ONE SYSTEM, ONE RECORD, ONE HAPPIER PATIENT
Announced in January, the three-pronged attack on data siloes and fragmentation starts with Coming Together, a feature that allows users to find and integrate patient records from other organizations – including those that do not use Epic.
“We can pull data from almost anywhere,” said Faulkner, “and we can allow our users to extend their systems into places that might not even have EHRs. All you need is an internet connect to use Epic Care Link, for example. It’s a web-based tool that allows other providers of the patient to schedule appointments, place orders, make referrals, and send data.”
Epic’s standards-based exchange tools, such as Care Everywhere, contribute to the movement of data across organizational lines, she added. “If it’s an Epic-to-Epic exchange, we can share 415 data elements. If it’s Epic to another vendor, we can exchange whatever people send us, but it’s typically much less.”
Avoiding data overload and cognitive fatigue when trying to synthesize information from multiple sources is the next step, said Faulkner.
“That’s where Happy Together comes in,” she said. “You only have a certain number of minutes for every appointment, and you simply can’t take the time to go somewhere else to see the data that you might need.
“Happy Together puts it all together as if it was from the same organization: here are all the test results and all the visits for the patient – but there’s a little symbol next to everything coming from the outside, and you can see where it’s coming from.”
The third piece of the puzzle, Working Together, furthers the goal of allowing providers to act in concert with one another.
“Working Together does things like let you see a thumbnail image from everywhere the images are available,” said Faulkner. “If you click on it, we go back to the original site where it was created, pull in a large image, and present it to you in that workflow. It’s reference quality right now – shortly we will have diagnostic quality.”
“You can also book appointments in another system, and message back and forth with that provider. Right now, when you get a referral to a specialist, you typically have to make the appointment or have that organization call you to make the appointment later. Now the referring provider can make it right away, which reduces a lot of pain points.”
INCLUDING THE PATIENT VOICE IN THE PATIENT’S CARE
Striking the right balance between patient control and provider involvement in the comprehensive health record is a challenge, she acknowledged.
Empowering patients to make better decisions about their own health is a critical part of effective population health management and a key component of addressing the social determinants of health – and yet patients cannot be left on their own to manage something as important and extensive as their entire health data history.
“One patient record held by a patient isn’t going to work,” said Faulkner. “Patients are busy, and they’re not going to be able to update their records and manage all that information between the kids and their jobs and not feeling well.”
“You only have a certain number of minutes for every appointment, and you simply can’t take the time to go somewhere else to see the data that you might need."
“It’s not going to be good quality data if we leave it entirely to the individual. It needs to be curated and cared for by the health systems, but the patient needs to have as much input and control as possible.”
Integrating the patient voice into the record can be accomplished by treating the patient portal as an essential part of care and communication instead of an afterthought simply required to meet meaningful use.
Epic has expended a great deal of effort on making its MyChart patient portal a pillar of the patient-provider relationship. With new educational resources from the Mayo Clinic, a single instance of the portal for patients visiting multiple Epic sites, and a range of self-assessment tools available to help patient take charge, the app allows providers to accept significant patient-generated feedback.
“Patients can contribute a lot of the data we need about social determinants themselves,” said Faulkner. “That’s why we have questionnaires in MyChart that are automatically pulled into the record.”
“The patient often prefers doing it themselves rather than answering questions from a provider, because they can take their time and figure out how they want to answer and what they want to say.”
Such patient-generated health data will help providers fill in the gaps when it comes to socioeconomics, patient self-care capabilities, health literacy, and the availability of social and community support to promote healthy behaviors.
Armed with this information, providers will be better able to treat patients as comprehensively as their health IT systems are starting to do.
“As more and more data is being collected, there’s more and more we can think of to deliver the best possible care to everyone,” said Faulkner.
“And as we get past the basics of working with the software, then we can leverage it better. If you want to do that, you have to think about being comprehensive when you’re designing the tools you need to care for patients in a holistic way.”